![[Current Topics in Psychology]](http://www.psychservices.com/CTparent.jpg)
American Psychological Association
119th Annual Convention - Washington, D.C.
August 4-7, 2011
These edited reports were originally posted to the Current Topics, Therapy Online, and Cyberpsychology list-servs, August 2011.
2011 Convention Highlights:
2011: eHealth Odyssey | Googling, Twittering, Poking | Zimbardo: Reflections + Enduring Lessons from 40 Years Ago: Stanford Prison Experiment Opening Ceremony/Keynote
Avatar-based Treatments | Canine Cognition: Chaser | Aaron T. Beck @90 | CCBT | Seligman: Flourish | Psychology, Technology, Virtual & Augmented Reality | Relationships 3.0
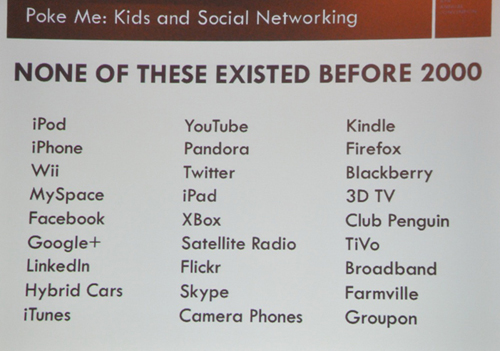
POKE ME: How Social Networks Can Both Help and Harm Our Kids | 'Monastic' Psychology Studies | Telehealth and Telepsychology Licensure - Barriers and Possible Solutions
![[color line]](http://www.fenichel.com/moveline.gif)
![[Capitol Building at Dusk - APA 2011]](http://www.fenichel.com/dc11-mini.jpg)
 The "Net Lounge", with Wifi, charging stations, family areas, and applications
The "Net Lounge", with Wifi, charging stations, family areas, and applications



CONVERSATION HOUR #3103 - A Very Special Event


"Virtual Reality integrates realtime computer processing, interface technology, body tracking & sensory displays to support a user to interact with and/or become immersed in a computer generated simulated environment. Within such controllable, dynamic and interactive 3D stimulus environments, behavioral action can be motivated, recorded and measured."





| Virtual Reality Definitions |
|---|
TechnoCentric Definition: "Virtual Reality integrates realtime computer processing, interface technology, body tracking & sensory displays to support a user to interact with and/or become immersed in a computer generated simulated environment. Within such controllable, dynamic and interactive 3D stimulus environments, behavioral action can be motivated, recorded and measured." |
|
HumanCentric Definition: "...a way for humans to interact with computers and extremely complex data in a more naturalistic fashion." |

THE SOLUTION:
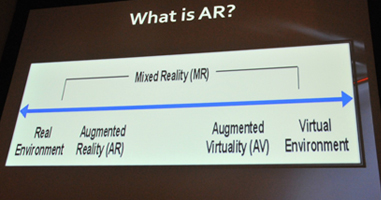
Augmented Reality- is a process by which digital images are overlaid upon real world spaces - combines real and virtual images into one 3D display - lets people interact and manipulate these digital images as if they were in real space |





| Basic Facts About Licensure |
|---|
* Professions are regulated by the States * There is no 'national' License * Most laws have transitioned from title to practice acts "You can NOT do the things described as being within the purview of a profession." - unless you are licensed to practice that profession. If someone says they are a “life coach” but is providing psychological services, they are practicing psychology, "whether they call themselves a psychologist or not." "LICENSING LAWS ARE DESIGNED TO PROTECT THE PUBLIC, NOT THE PROFESSION" |
What is License Portabilty?
A system that extends the privilege to practice a health profession in multiple states through agreements that recognize individual state and territorial jurisdiction while facilitating a process for obtaining and maintaining licenses in multiple jurisdictions.
